Cap-dependent endonuclease inhibitor Baloxavir marboxil (Xofluza®)
Introduction
1. Action mechanism of baloxavir marboxil
2. Administration method and dosage of baloxavir marboxil
3. Clinical efficacy similar to that of oseltamivir orally administered
4. Adverse reactions
5. Appearance of amino acid mutations
6. Marked reduction in the virus titer
Conclusion
Introduction
In March 2018, a new anti-influenza drug, baloxavir marboxil (Xofluza®), became commercially available. It reduces viral proliferation by inhibiting cap-dependent endonuclease, which is a new action mechanism, different from conventional neuraminidase inhibitors. As treatment with this drug is completed by single-dose oral administration, it may be clinically useful. However, this drug is known to frequently induce viral amino acid mutations. In the future, the influence of such mutations on the clinical effects and infectivity must be examined.
This drug may be used in earnest in prevalence this winter. Here, we introduce the characteristics of this drug, which are also shown in the package inserts*.
* Package inserts of Xofluza® tablets 10 mg/20 mg and granule 2% portions, prepared by Shionogi & Co., Ltd. in September 2018 (3rd version)
http://www.info.pmda.go.jp/downfiles/ph/PDF/340018_6250047F1022_1_04.pdf
1. Action mechanism of baloxavir marboxil
Influenza viral infection occurs when hemagglutinin on the envelope surface binds to receptors on the cell surface of the human airway. Virus ribonucleoprotein (RNP) complex is released in the intracellular space (shelling), and migrates into the nucleus. Messenger RNA (mRNA) synthesis by viral RNA transcription and viral genome RNA replication are separately promoted. As an RNA polymerase inhibitor, baloxavir marboxil, inhibits mRNA synthesis. Viral polymerase consists of PA, PB1, and PB2. Baloxavir marboxil hinders mRNA synthesis by inhibiting the cap-dependent endonuclease of PA, suppressing virus proliferation.
On the other hand, viral neuraminidase cuts cell receptor-virus binding during proliferating virus expansion from the cellular area to its periphery (budding). Thus, neuraminidase inhibitors (NAIs) inhibit neuraminidase.
2. Administration method and dosage of baloxavir marboxil
Baloxavir marboxil is an oral preparation. For adults (including children aged ≥12 years), two 20-mg tablets (total: 40 mg) or 4 portions of granule should be administered once on the first day of treatment (4 tablets (80 mg) or 8 portions of granule to patients weighing ≥80 kg). For children aged <12 years, two 20-mg tablets (40 mg) or 4 portions of granule should be administered to those weighing ≥40 kg, a 20-mg tablet (20 mg) or 2 portions of granule to those weighing 20 to 39 kg, and a 10-mg tablet (10 mg) to those weighing <20 kg. Treatment is completed after single-dose administration, characteristic of this drug.
The teratogenicity of baloxavir marboxil has not yet been demonstrated, but treatment with this drug should be avoided in pregnant women (in the package inserts, it is recommended that this drug should be carefully administered).
Baloxavir marboxil is primarily excreted in feces (80%), and it can be used without regulating the dose even in patients with kidney hypofunction.
3. Clinical efficacy similar to that of oseltamivir orally administered
The results of a clinical study involving outpatients who consulted a hospital within 48 hours after onset were reported, with respect to baloxavir marboxil use.
Baloxavir marboxil is effective for influenza A/B virus infection. In vitro studies confirmed that this drug was effective for avian influenza H5N1 and H7N9, and clinical studies demonstrated the efficacy of this drug for influenza H1N1pdm09 and A Hong-Kong (H3N2) viral infection.
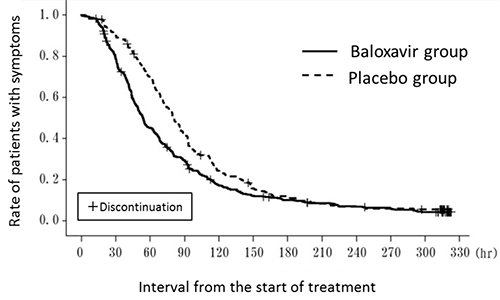
In an international, cooperative phase III study involving adults, the duration of disease for placebo and baloxavir groups was 80.2 and 53.7 hours, respectively, showing a significant 26.5-hour reduction (Figure 1). In adults, a comparative study using oseltamivir as a control drug was conducted, but the effects on clinical symptoms were similar between the two drugs.
A phase III clinical study involving children (aged <12 years) in Japan showed that the median interval until symptom relief was between 40 and 60 hours. This study involved children who were able to take tablets, but a clinical trial of a granule preparation was also completed, and granule preparation may be primarily used for young children in the future.
Figure 1. Kaplan-Meier curve in an international, cooperative phase III study
Package inserts of Xofluza® tablets 10 mg/20 mg and granule 2% portions, prepared by Shionogi & Co., Ltd. in September 2018 (3rd version)
http://www.info.pmda.go.jp/downfiles/ph/PDF/340018_6250047F1022_1_04.pdf
4. Adverse reactions
Adverse reactions, including abnormal laboratory data, were observed in 5.4% (49/910 patients) of adults (including children aged ≥12 years) in a clinical study. Primarily, diarrhea and an increase in ALT level were noted.
In a clinical study involving children aged <12 years, adverse reactions were observed in 3.8% (4/105 patients). No serious adverse event has been reported in any adult or child.
5. Appearance of amino acid mutations
In a phase III clinical study involving Japanese children, amino acid mutants were detected in 18 (23.3%) of the 77 patients in whom base-sequence analysis was possible before and after the administration of baloxavir marboxil. Those patients had influenza A.
In a clinical study involving adults, mutations were detected in 36 (9.7%) of 370 patients. The 38th amino acid of the PA gene, isoleucine (I), is substituted for threonine (T), and termed I38T (I38F and I38M were also detected in addition to I38T). The appearance of I38T mutant virus reduced the susceptibility of the influenza virus to baloxavir marboxil about 50-fold. However, the rate of reduction in the susceptibility is relatively small, and some investigators consider the term "low-susceptibility virus", rather than "resistant", appropriate.
Treatment with baloxavir marboxil frequently induces mutations, but their influence on clinical effects remains uncertain. For example, the H275Y mutation of H1N1pdm09 (the 275th amino acid of the neuraminidase gene NA1, histidine, is substituted for tyrosine), which transiently became prevalent in Hokkaido, reduced the susceptibility of the virus to oseltamivir 200- to 300-fold. However, no study has reported a reduction in the clinical effects. During susceptibility tests, neuraminidase inhibition assay for NAIs is performed, and plaque reduction assay for baloxavir marboxil is conducted; different methods are used.
Although it is impossible to simply compare the reduction of susceptibility between the two drugs, we cannot conclude that the resistance level is low, or that the influence on clinical effects is slight based on the rate of reduction in the susceptibility to baloxavir marboxil (about 50-fold). These issues must be examined from basic and clinical viewpoints in the future.
The infectivity of the I38 mutant virus is also unclear, but one study confirmed that mutations reduced the virus' proliferation capacity (Omoto S, et al., Scientific reports 2018; 8:9633). The influence of amino acid mutations on clinical effects should be investigated in the future.
6. Marked reduction in the virus titer
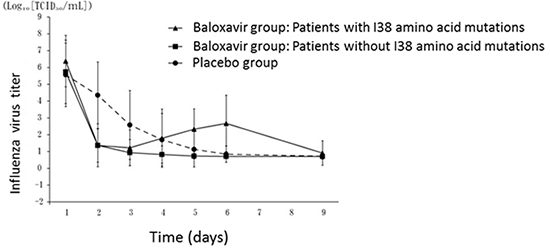
In an international, cooperative phase III clinical study, the virus titer was approximately 6 (log10 TCID50/mL) before administration, but markedly reduced to approximately 2 the day after administration (Figure 2). This suggests a rapid decrease in the nasopharyngeal level of influenza virus. As the nasopharyngeal virus level may reflect its infectivity, it is possible that day 2 levels may continue to be reduced following treatment with baloxavir marboxil. In many cases, the results of rapid diagnosis may become negative the day after baloxavir administration. On the other hand, in patients treated with NAIs, such as oseltamivir, the virus titer does not markedly reduce even after the start of treatment; therefore, the results of rapid diagnosis remain positive.
The clinical efficacy of baloxavir marboxil is similar to that of oseltamivir, but the anti-viral activity of the former is markedly more potent than that of the latter.
In patients for whom I38 mutant virus was detected, an additional increase in the virus titer 4 to 5 days after baloxavir administration was observed (Figure 2). The titer, which rapidly reduced the day after baloxavir administration, again increased to approximately 2 to 3 (log10 TCID50/mL). According to a recent study (Hayden FG, et al., N Eng J Med 2018; 379:913), the duration of disease (median time to alleviation of illness) in patients in whom I38 mutant virus was detected was prolonged in comparison to those without mutations; it was 49.6, 63.1, and 80.2 hours, respectively, in the mutation (-), I38 mutation (+), and placebo groups.
Figure 2. Changes in the virus titer with respect to the presence or absence of I38 amino acid mutations in an international, cooperative phase III study
Package inserts of Xofluza® tablets 10 mg/20 mg and granule 2% portions, prepared by Shionogi & Co., Ltd. in September 2018 (3rd version)
http://www.info.pmda.go.jp/downfiles/ph/PDF/340018_6250047F1022_1_04.pdf
According to the above study (N Eng J Med), the virus was detected in 7% of mutation-free patients, in 91% of those with mutations, and in 31% of placebo-treated patients 5 days after the start of treatment, and in 2%, 17%, and 6%, respectively, 9 days after its start.
Conclusion
As baloxavir marboxil (Xofluza®) suppresses the proliferation of influenza virus via an action mechanism different from NAIs, it may be effective against NAI-resistant viruses. The clinical efficacy (duration of influenza illness) of this drug is similar to those of oseltamivir. However, treatment can be completed by single-dose oral administration; therefore, the availability of this drug is high, and adherence is favorable.
In addition, this drug markedly reduces the virus titer in the early phase; therefore, it is therapeutic and possibly leads to the prevention of the transmission of influenza virus to one's surroundings. However, it was reported that amino acid mutations (primarily I38T) frequently developed (children: 23.3%, adults: 9.7%). The susceptibility of mutant virus to baloxavir marboxil is reduced by approximately 50-fold, but the influence on clinical effects and infectivity remain uncertain. In the future, the positioning of this drug must be established by accumulating clinical cases.
December 1, 2018
Influenza Committee of The Japanese Association for Infectious Diseases
Yosuke Aoki, Akihiko Kawana, Hiroyuki Kunishima, Masayoshi Shinjoh, Norio Sugaya, Hideaki Nagai, Nobuo Hirotsu, Jiro Fujita, Hiroshige Mikamo & Tadashi Ishida (Chairperson of the committee)
Self-reported Potential Conflict of Interest Disclosure Statement
Dr. Yosuke AOKI received lecture fees from MSD K.K.., Taisho Toyama Pharmaceutical Co., Ltd., and Pfizer Japan Inc.
Dr. Yosuke AOKI received scholarship donations from Shionogi & Co., Ltd., and MSD K.K.
Dr. Hiroyuki KUNISHIMA received lecture fees from MSD K.K., Taisho Toyama Pharmaceutical Co., Ltd., and Toyama Chemical Co., Ltd.
Dr. Hiroyuki KUNISHIMA received research funds from Becton, Dickinson and Company.
Dr. Norio SUGAYA received lecture fees from Astellas Pharma Inc., Shionogi & Co., Ltd., and Chugai Pharmaceutical Co., Ltd.
Dr. Hideaki NAGAI received lecture fees from MSD K.K., and Pfizer Japan Inc.
Dr. Nobuo HIROTSU received lecture fees from Shionogi & Co., Ltd.
Dr. Jiro FUJITA received lecture fees from MSD K.K., Shionogi & Co., Ltd., Daiichi Sankyo Co., Ltd., Taisho Toyama Pharmaceutical Co., Ltd., Pfizer Japan Inc., and Nippon Boehringer lngelheim Co., Ltd.
Dr. Jiro FUJITA received research funds from KYORIN Pharmaceutical Co., Ltd.
Dr. Jiro FUJITA received scholarship donations from Eisai Co., Ltd., MSD K.K., Otsuka Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Taiho Pharmaceutical Co., Ltd., Toyama Chemical Co., Ltd., Pfizer Japan Inc., Nippon Boehringer lngelheim Co., Ltd., and Meiji Seika Pharma Co., Ltd.
Dr. Hiroshige MIKAMO received rewards as a medical advisor from Toyama Chemical Co., Ltd.
Dr. Hiroshige MIKAMO received lecture fees from Asahi Kasei Pharma Corporation, Astellas Pharma Inc., MSD K.K., Shionogi & Co., Ltd., Daiichi Sankyo Co., Ltd., Taisho Toyama Pharmaceutical Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Toyama Chemical Co., Ltd., Pfizer Japan Inc., Miyarisan Pharmaceutical Co., Ltd., and Meiji Seika Pharma Co., Ltd.
Dr. Hiroshige MIKAMO received a manuscript fee from MSD K.K., and Taisho Toyama Pharmaceutical Co., Ltd.
Dr. Hiroshige MIKAMO received research funds from EIDIA Co., Ltd., Otsuka Pharmaceutical Factory, Inc., KYORIN Pharmaceutical Co., Ltd., Saraya Co., Ltd., Taisho Pharmaceutical Co., Ltd., Tosoh Corporation, Becton, Dickinson and Company, Bayer Yakuhin, Ltd., Precision System Science Co., Ltd., and Miyarisan Pharmaceutical Co., Ltd.
Dr. Hiroshige MIKAMO received scholarship donations from Asahi Kasei Pharma Corporation, Astellas Pharma Inc., Eneforest Co., Ltd., MSD K.K., Shionogi & Co., Ltd., Daiichi Sankyo Co., Ltd., Taisho Toyama Pharmaceutical Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Toyama Chemical Co., Ltd., Pfizer Japan Inc., FUJIFILM Holdings Corporation, Miyarisan Pharmaceutical Co., Ltd., and Meiji Seika Pharma Co., Ltd.
Dr. Tadashi ISHIDA received lecture fees from MSD K.K.
